Normal Ultrasound But Still Endometriosis Pain?
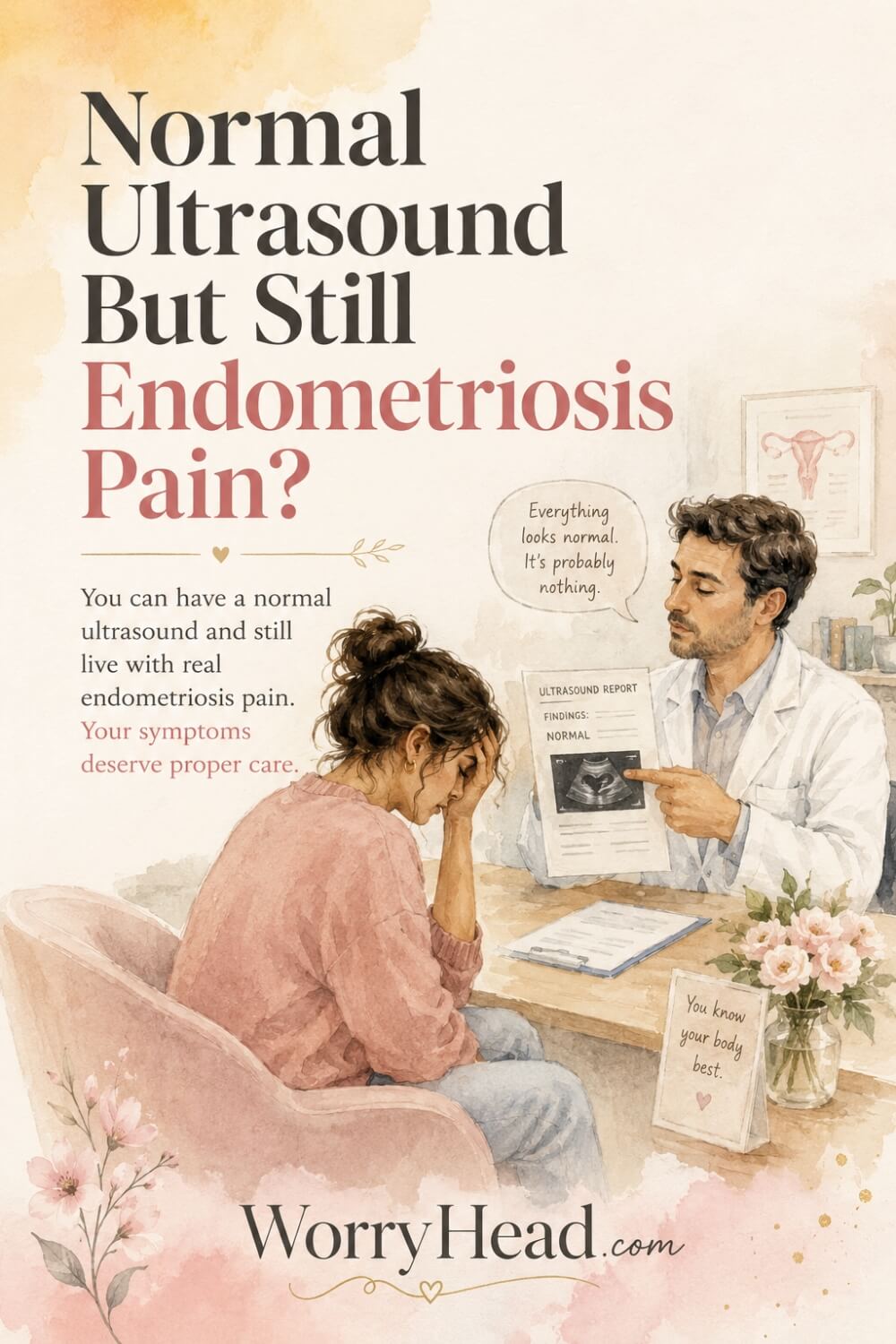
Have you been told your scan looks normal, but your body is still screaming in a way you cannot explain? This is exactly why a normal ultrasound but still endometriosis pain can feel so confusing, frightening, and unfair. You are not overreacting. You are not being dramatic, and a clean-looking scan does not automatically mean your pain has no real cause.
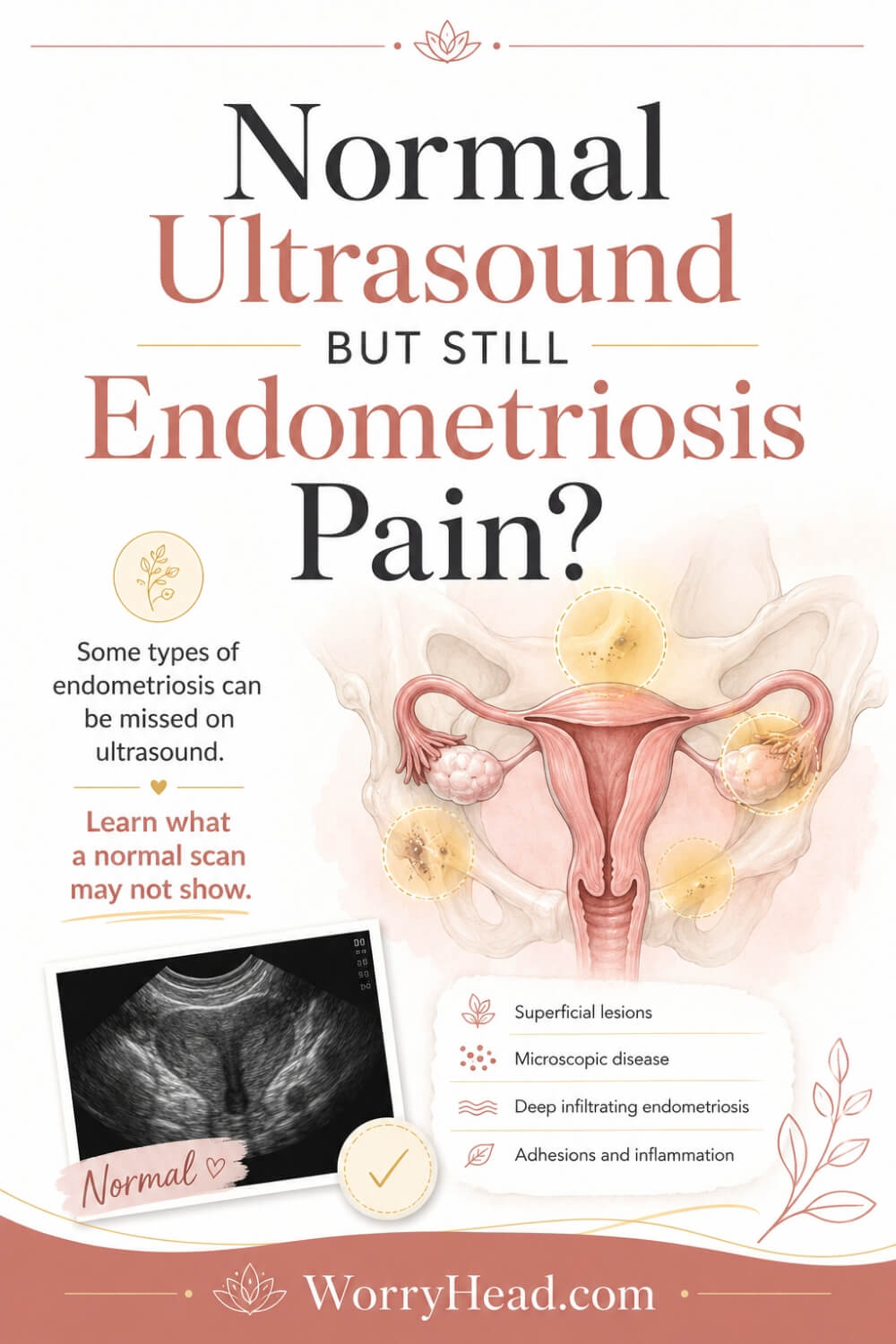
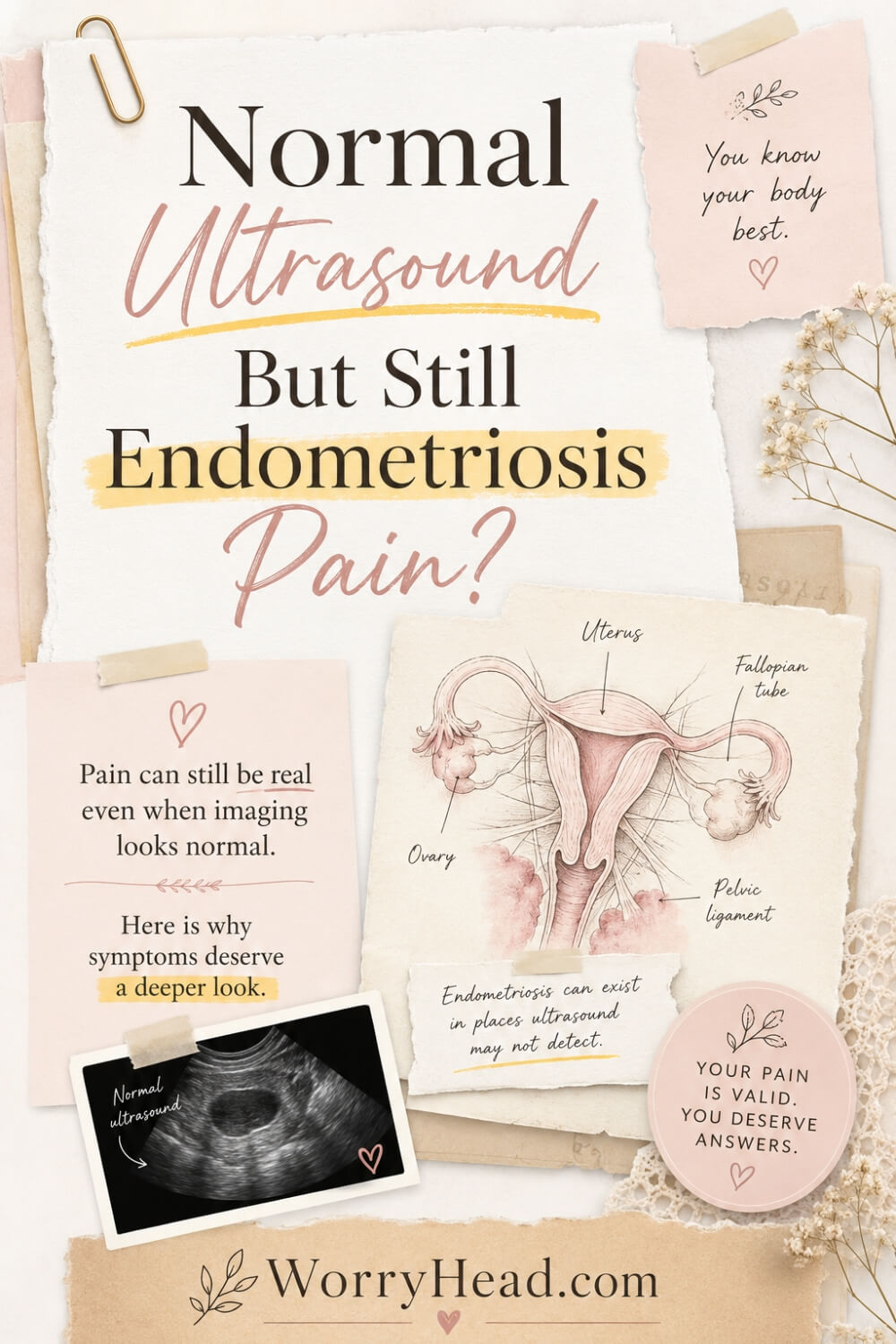
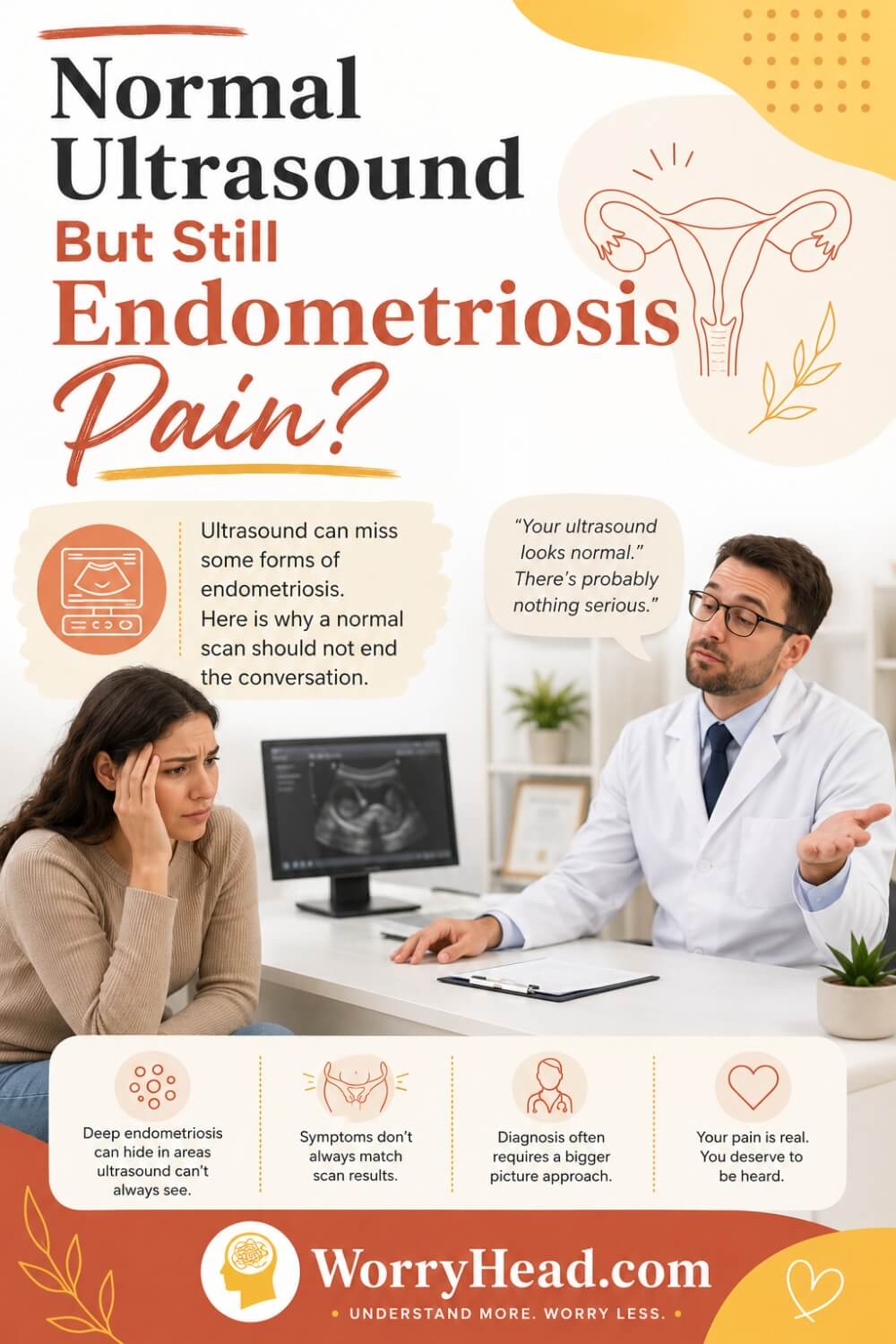
A normal ultrasound can miss endometriosis, especially superficial peritoneal disease, tiny lesions, adhesions, or deep disease not scanned by an expert. Your pain still matters, and ongoing symptoms deserve review, referral, specialist imaging, or laparoscopy if needed, not dismissal today.
I am not a clinician, but I have seen with my own eyes, and heard thousands of stories of medical gaslighting of endometriosis. I write as a husband, blogger, and researcher who has spent years learning because of my wife. Not everything is gaslighting, so at the bottom of this article I have attached the sources I used to understand the medical context, including WHO, NICE, NHS, ESHRE, and published studies.
What surprises many people is that ultrasound is not useless, but it is not magic either. NICE recommends transvaginal ultrasound for suspected endometriosis because it can help find ovarian endometriomas, deep endometriosis involving places like the bowel, bladder, or ureter, and other causes of pelvic pain, but NICE also says endometriosis should not be excluded when the scan is normal.
ESHRE also explains that negative imaging does not exclude endometriosis, especially superficial peritoneal disease, and that laparoscopy may still be considered when imaging is negative, or treatment has not helped. The World Health Organization describes endometriosis as a chronic disease affecting about 10% of reproductive-age women worldwide, around 190 million people, with symptoms that can include severe period pain, chronic pelvic pain, painful bloating, nausea, heavy bleeding, and infertility.
I have seen how something as short as “normal scan” can land like a slap when my wife is still curled up in pain, trying to explain a body that keeps interrupting her life. As her husband, I learned that the most loving thing I could do was not to question her pain, but to question the gap between her symptoms and the answer she was given.
If this already feels like something you needed to hear, I invite you to grab my FREE 130+ page eBook, “You Did Nothing To Deserve This!”, written to validate the feelings of women living with endometriosis. By grabbing it, you also join our community, where I share more freebies, big discounts on all our books, and honest, helpful emails about adjusting to the new normal chronic illness can bring into your relationship and life.
The book is filled with 20 chapters of gentle validation for women with endo, written by yours truly, as I have seen it up close...
- This Was Never Your Fault
- The Girl You Used To Be
- When Your Own Body Feels Like an Enemy
- The Invisible Battles Nobody Sees
- Am I Just Lazy? – The Lie You Have Been Taught
- Gaslighting, Dismissal and the Trauma of Not Being Believed
- Guilt: The Weight You Were Never Meant to Carry
- Love in the Middle of Pain
- Intimacy When Your Body Hurts
- The Loneliness of Being the Strong One
- You Are Allowed To Take Up Space
- Tiny, Gentle Hopes (Not Toxic Positivity)
- If You Could Hear My Voice Every Flare Day
- You Deserve Partners, Not Witnesses
- When You Wish He Understood
- Motherhood, Fertility and the Grief Nobody Sees
- When Anger Is the Only Honest Feeling
- Learning to Trust Your Body Again
- Building a Life That Fits Your Reality
- You Did Nothing To Deserve This
You Did NOTHING To Deserve This!
Endometriosis Validation for Women with Endo
- You Did NOTHING To Deserve This!
- Why a Normal Ultrasound But Still Endometriosis Pain Can Happen?
- Why Normal Ultrasound But Still Endometriosis Pain Should Never Be Dismissed?
- How Normal Ultrasound But Still Endometriosis Pain Changes Your Relationship With Your Body?
- When to Seek Medical Help?
- Questions to Ask Your Doctor
- Final Word on Normal Ultrasound But Still Endometriosis Pain
- FREE eBook
Why a Normal Ultrasound But Still Endometriosis Pain Can Happen?
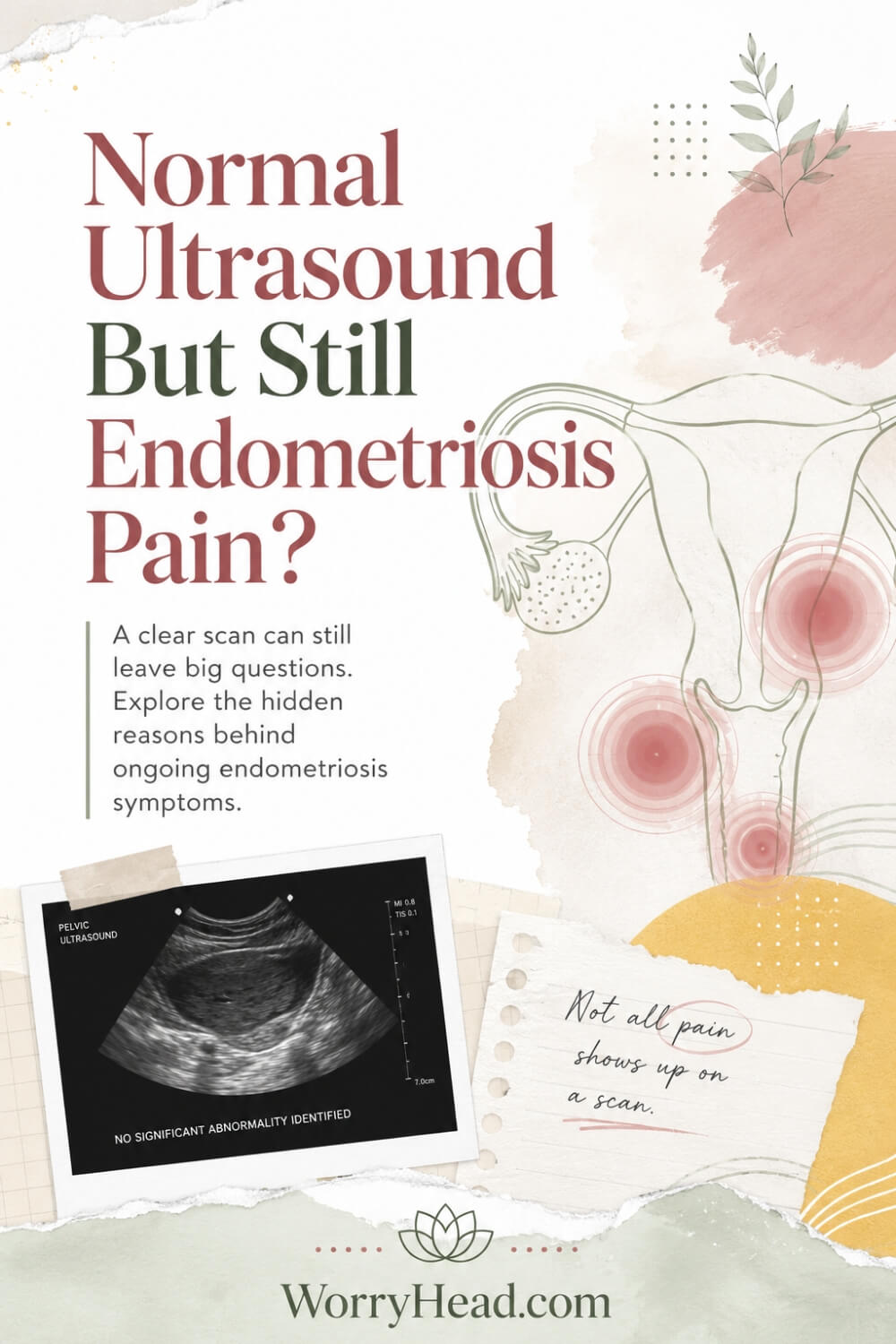
A normal ultrasound but still endometriosis pain story usually begins with a sentence that sounds reassuring to the clinician but devastating to the person still hurting. The scan may show normal-looking ovaries, uterus, and pelvic structures, yet that does not prove your symptoms are imagined or harmless.
NICE guidance says endometriosis should not be ruled out just because the abdominal or pelvic examination and ultrasound are normal, and referral may still be needed when symptoms continue.
Ultrasound is helpful, but it sees some forms of disease better than others. It can help identify ovarian endometriomas and deep endometriosis involving areas such as the bowel, bladder, or ureter, but superficial peritoneal endometriosis can be much harder to detect.
This matters because pain is not always proportional to what appears on a scan. Mayo Clinic explains that a small amount of endometriosis can cause severe pain, while someone with more visible disease may have little pain or no pain at all. That one fact alone should make every dismissive appointment pause for a moment.
Endometriosis pain can come from inflammation, irritated nerves, adhesions, cysts, deep lesions, muscle guarding, bowel involvement, bladder irritation, painful sex, or pain signals that become more sensitive over time. The ultrasound may not show the whole story because the body is not a flat photograph; it is moving, reacting, tightening, bleeding, inflaming, and protecting itself.
That is why your symptom pattern matters so much. Pain before your period, pain during your period, pain after your period, painful bowel movements, pain when peeing, deep pelvic pressure, lower back pain, nausea, bloating, fatigue, pain with sex, and pain that affects your normal life all deserve to be taken seriously.
WHO describes endometriosis as a chronic disease that can cause severe menstrual pain, chronic pelvic pain, heavy bleeding, bloating, nausea, infertility, pain with sex, bowel symptoms, urinary symptoms, and mental health impact. So when you say, “But I still feel something is wrong,” that sentence can be medically important, not emotional noise.
A standard pelvic ultrasound may also depend on the person scanning, the equipment used, the report wording, and whether the scan was done by someone trained to look for deep endometriosis. NICE specifically says specialist ultrasound or pelvic MRI should be planned and interpreted by professionals with specialist expertise when assessing deep endometriosis.
This does not mean every pain after a normal scan is endometriosis. It means the answer should be careful, curious, and honest, not rushed, cold, or final.
Other causes of pelvic pain may still need considering, including adenomyosis, fibroids, ovarian cysts, pelvic inflammatory disease, irritable bowel syndrome, bladder pain syndrome, pelvic floor dysfunction, and nerve-related pain. A good clinician should not use one normal scan to close the door; they should use it as one piece of the bigger puzzle.
Current guidance also supports considering laparoscopy when endometriosis is suspected even if ultrasound or MRI is normal, especially when symptoms persist or treatment has not helped. ESHRE guidance also warns that negative imaging does not exclude endometriosis, particularly superficial peritoneal disease.
For you, this means you are allowed to ask what kind of ultrasound you had, what it was looking for, what it could not rule out, and what the next step should be. You are allowed to say, “My scan was normal, but my life is not normal.”
I remember watching my wife leave appointments with that quiet look in her eyes, the kind that said she had been heard politely but not truly believed. I could not take her pain away, but I could stop becoming another person she had to convince. So before we go deeper into what you can actually do next, I want to give you practical steps that help you protect your voice, organise your symptoms, and walk into the next appointment with more confidence.
- Track pain beyond periods
- Ask for specialist imaging
- Describe bowel and bladder symptoms
- Bring a symptom timeline
- Question dismissal calmly
- Consider pelvic floor involvement
- Discuss treatment options early
- Protect your emotional energy
- Bring your partner into care
Track Pain Beyond Periods
When your scan is normal, your symptom pattern becomes even more important because pain often tells a story that one image cannot tell. Do not only write “bad period pain” and leave it there, because endometriosis symptoms can appear before bleeding starts, during bleeding, after bleeding, around ovulation, after sex, during bowel movements, when your bladder fills, or when fatigue knocks you flat for days.
Track where the pain sits, how it feels, how long it lasts, what triggers it, what eases it, and what it stops you from doing. I have learned through my wife that the tiny details matter, because one sentence like “I get stabbing rectal pain before my period” can explain far more than “my pelvis hurts.”
Your notes do not need to be perfect or medical. They only need to be honest enough to help you walk into the next appointment with evidence that your life is being interrupted, not a vague complaint that can be brushed aside.
Ask for Specialist Imaging
A normal scan can depend on what type of scan you had, who performed it, what they were trained to look for, and whether anyone was specifically searching for signs of deep endometriosis, adhesions, endometriomas, or organs that do not move as freely as they should.
A quick standard ultrasound may check the womb and ovaries, but it may not fully map the pelvic sidewall, bowel, bladder, ureters, pouch of Douglas, uterosacral ligaments, or signs of reduced organ mobility. This is why asking about specialist transvaginal ultrasound or MRI can be reasonable when your symptoms continue.
You are not being difficult by asking, “Was this scan done by someone trained in endometriosis imaging?”
That question can change the whole tone of the conversation. My wife taught me that the right question can protect you from being handed a final answer when you were only given a first step. A normal report should not become a locked door when your body is still giving distress signals.
Describe Bowel and Bladder Symptoms
Many people feel embarrassed to talk about bowel and bladder symptoms, but these details can be extremely important when endometriosis is suspected. Painful bowel movements, rectal pressure, diarrhoea around your period, constipation that follows your cycle, pain when your bladder fills, urinary urgency, burning without infection, or pain after peeing are not random details you should hide because they feel awkward.
They may help show whether pain is connected to pelvic nerves, inflammation, deep lesions, muscle guarding, or organs being irritated by nearby disease. I know these conversations are not easy, especially when you already feel exposed, tired, and frightened of being dismissed again.
But please remember this: your dignity is not reduced by describing what your body is doing. A good doctor needs the real picture, not the polite version. My wife spent years normalising things she should never have had to normalise, and that is why I want you to speak clearly, even if your voice shakes.
Bring a Symptom Timeline
A symptom timeline helps your doctor see patterns instead of isolated complaints.
Write down when your pain started, whether it worsened over months or years, what your periods are like, whether pain appears outside bleeding, and whether symptoms affect work, sleep, intimacy, digestion, bladder habits, mood, or daily movement. Include previous scan results, medication tried, hormonal treatment responses, pain relief that failed, emergency visits, fertility concerns, and days when you had to cancel life because your body would not let you function.
This does not need to look professional. A simple page with dates, symptoms, and impact can be powerful because it shows the difference between “I get cramps” and “I lose several days of my life every month.” I have seen how easily pain is minimised when it is spoken in fragments.
A timeline helps you bring the whole story into the room, even when you are exhausted and forget half of it under pressure.
Question Dismissal Calmly
Being calm does not mean accepting dismissal. It means protecting your energy while making it harder for your concerns to be brushed aside. You can say, “I understand the ultrasound was normal, but what does it not rule out?” or “Given my symptoms, what is the next step if endometriosis is still possible?”
These questions are respectful, but they also gently force the appointment back towards clinical reasoning rather than reassurance without explanation. I wish my wife had been given this kind of language earlier, because pain can make you feel small in a room where someone else controls the answers. You should not have to fight to be believed, but sometimes you do need phrases that keep the door open. If you feel dismissed, ask for the reasoning to be written in your notes, ask what red flags to watch for, and ask when you should come back if symptoms continue. That is not drama. That is self-protection.
Consider Pelvic Floor Involvement
Endometriosis pain is not always only about lesions. When pain repeats for months or years, the pelvic floor muscles can start guarding, tightening, and reacting as if they are trying to protect you from the next flare.
This can add deep pelvic aching, pain with sex, bladder urgency, bowel difficulty, tailbone pain, hip pain, or a feeling that everything inside is clenched and unsafe.
A normal ultrasound will not show how much your muscles are guarding or how sensitised your nervous system has become. That does not make the pain less real. It simply means the pain picture may involve more than one layer.
My wife’s pain taught me that the body can remember suffering, and sometimes it keeps bracing long after the original trigger has passed. Asking about pelvic floor physiotherapy, pain management, or a clinician who understands chronic pelvic pain can be a practical next step, not an admission that the pain is “all in your head.”
Discuss Treatment Options Early
You do not have to wait until every test is dramatic before discussing treatment. Depending on your symptoms, medical history, fertility plans, and preferences, your clinician may talk about pain relief, hormonal options, referral to gynaecology, specialist imaging, pelvic physiotherapy, or laparoscopy if symptoms persist and endometriosis remains suspected.
What matters is that you are part of the decision, not pushed into something without understanding the benefits, limits, and trade-offs. Ask what the goal of each option is: symptom control, diagnosis, fertility planning, reducing flares, or improving quality of life. Also ask what happens if the first option does not help.
I say this because my wife’s life was never a textbook pathway. It was messy, emotional, and full of decisions that affected both her body and our relationship. You deserve care that sees you as a whole person, not a scan result with legs.
Protect Your Emotional Energy
A normal scan after months or years of pain can feel like being told your suffering has nowhere to live. That can break something inside you, especially if you were secretly hoping the scan would finally prove what you already feel.
Please do not measure your truth by the neatness of a report. Pain that changes your day, your work, your sleep, your intimacy, your confidence, and your sense of safety in your own body deserves compassion. I have watched my wife become quiet after appointments, not because she had nothing to say, but because she was tired of explaining pain to rooms that kept looking for easier answers.
Protect your emotional energy by bringing someone with you, writing questions beforehand, resting after appointments, and reminding yourself that not being diagnosed yet is not the same as being wrong. You are allowed to feel angry, sad, confused, and still keep going.
Bring Your Partner Into Care
If you have a partner, bring them into the reality of what you are living with, not just the appointment room. Let them see the pattern, the fatigue, the fear before bleeding starts, the way pain changes your face, the way you push through because you do not want to disappoint anyone.
A loving partner should not need perfect medical proof before offering tenderness. I say that as a husband who had to learn, sometimes painfully, that support is not only driving to appointments or buying tablets. Support is believing her before the world confirms her. It is listening when she says something is wrong. It is not taking her exhaustion personally. It is learning enough to stand beside her without speaking over her.
If you are reading this as the person in pain, you deserve that kind of support. If you are reading this as the partner, please understand that your belief may become the safest place she has while medicine catches up.
Why Normal Ultrasound But Still Endometriosis Pain Should Never Be Dismissed?
Normal ultrasound but still endometriosis pain should be taken seriously because imaging is only one part of the diagnosis, not the full story of your body. NICE says suspected endometriosis should not be ruled out just because the examination and ultrasound look normal, and ESHRE warns that negative imaging does not exclude endometriosis, especially superficial peritoneal disease.
That matters because a scan can miss what your daily life cannot miss. It cannot measure the dread you feel before your period arrives, the way bowel pain makes you grip the bathroom sink, or the quiet fear that comes when sex, work, sleep, and simple plans start revolving around pain.
I have watched my wife try to stay graceful through symptoms that would make many people collapse, and I know how cruel it sounds when a report says “normal” while your face says “I am barely coping.” A report can describe what was seen on that day, by that machine, through that operator’s eye, but it cannot describe the whole pattern of your suffering.
The NHS lists symptoms such as pelvic pain, pain when you poo or pee, pain during or after sex, extreme tiredness, fertility difficulties, low mood, and anxiety as possible parts of endometriosis. When your symptoms line up with that kind of pattern, your next step should not be shame, silence, or pretending you are fine.
It should be a careful conversation about what the scan could see, what it could not see, whether specialist imaging is needed, and whether referral to gynaecology or an endometriosis centre makes sense. NICE also says laparoscopy can be considered to diagnose suspected endometriosis even when ultrasound or MRI is normal, which is important when pain continues despite reassurance.
I wish more partners understood this, because belief at home can become the bridge between being dismissed and being helped. When my wife could not find the strength to explain everything again, I learned to remember the details, notice the patterns, and gently remind her that she did not need to earn my compassion with medical proof.
Your pain deserves that same steadiness. You deserve someone who says, “I believe you,” before the system finally catches up, because a normal scan may calm a clinic, but it does not automatically calm the body living through the pain.
How Normal Ultrasound But Still Endometriosis Pain Changes Your Relationship With Your Body?
Normal ultrasound but still endometriosis pain can slowly make you doubt your own body, even when your symptoms are controlling your day. The NHS lists pelvic pain, difficult periods, pain during or after sex, pain when peeing or pooing, extreme tiredness, and fertility problems as symptoms that can come with endometriosis, so your experience may be far bigger than what one scan report can hold.
I have seen this doubt in my wife’s face, and it is one of the things that hurts me most as her husband. Pain already steals enough from her, but dismissal adds another wound because it makes her wonder whether she is asking for too much when she is actually asking for basic understanding.
For her, the hardest part was not only the pain itself, but the way it interrupted ordinary life without warning. A plan could become impossible, a meal could become uncomfortable, intimacy could become complicated, and a normal day could suddenly shrink into surviving the next hour.
For me, it changed the way I understood love. I learned that support is not only saying “I’m here”, ” but it is also noticing when her breathing changes, remembering what happened after the last flare, and refusing to let a normal-looking result make me careless with her suffering.
For both of us, it affected trust, closeness, patience, and the quiet rhythm of our home. It taught me that endometriosis is not only a gynaecological condition on paper, but a daily relationship with uncertainty, appointments, pain relief, fear, hope, and the need to be believed before everything is medically proven.
NICE guidance now clearly says suspected endometriosis should not be excluded just because the examination or ultrasound is normal, which matters because it protects you from being pushed into silence too early. If your life is still being interrupted, your next step is not to blame yourself, but to keep the conversation open, ask for proper review, and let your symptoms be taken seriously.
When to Seek Medical Help?
Please do not wait until you are completely broken before asking for help again. If your ultrasound was normal but your pain keeps coming back, keeps worsening, or keeps interfering with your work, sleep, sex life, digestion, bladder, mood, or ability to live normally, that is enough reason to speak to a doctor.
A normal scan can be reassuring for some things, but it does not close the whole endometriosis conversation. NICE guidance says suspected endometriosis should not be excluded just because an examination or ultrasound is normal, and referral may still be needed if symptoms continue.
I would seek medical help if your periods are so painful that you plan your life around them, if painkillers barely touch the pain, if you regularly need time off work or school, or if you find yourself dreading your cycle before it even starts. Pain that repeatedly steals normal days from you deserves more than “come back if it gets worse.”
You should also ask for help if you have pain when you poo or pee, deep pain during or after sex, bleeding from the bowel around your period, bladder urgency, lower back pain, leg pain, pelvic pressure, nausea, bloating, or fatigue that arrives with the pain pattern. The NHS lists pelvic pain, pain during or after sex, pain when pooing or peeing, extreme tiredness, fertility difficulties, low mood, and anxiety as symptoms that can occur with endometriosis.
If you are trying to conceive, worried about fertility, or you have been told “everything looks fine” while your body keeps telling you otherwise, please do not let embarrassment keep you quiet. Fertility worries carry a different kind of pain, one my wife and I understand deeply, because it does not only touch the body, it touches the future you quietly imagined.
There are also times when pelvic pain needs urgent help, not just a routine appointment. In the UK, NHS advice says to call 999 or go to A&E if pelvic pain is severe, getting worse, hurts when you move or touch the area, or comes with fainting, dizziness, shoulder-tip pain, difficulty breathing, heavy vaginal bleeding, or sudden confusion.
That is not written to frighten you. It is written because you deserve to be safe, and not every severe pelvic pain episode should be automatically blamed on endometriosis, even when you already suspect it.
If you are pregnant, might be pregnant, or there is any chance of pregnancy, pelvic pain and bleeding should be taken seriously and checked quickly. Pain in early pregnancy can have different causes, and some need urgent assessment, so this is one of those moments when it is better to be cautious than brave in silence.
For ongoing symptoms, I would book a GP appointment, ask for a referral to gynaecology, and explain how your symptoms affect your life, not only where the pain is. Say things like, “I cannot work normally,” “I avoid sex because of deep pain,” “I get bowel pain around my period,” or “My scan was normal, but my symptoms are still controlling my life.”
I have learned from my wife that the body often whispers for years before it screams. Please do not wait for the scream before you ask someone to listen properly.
Questions to Ask Your Doctor
When you sit in front of a doctor after a normal scan, it can be hard to think clearly. Pain, nerves, past dismissal, and the fear of being made to feel dramatic can make your mind go blank, so I would write your questions down before the appointment.
You are not there to argue. You are there to understand what has been ruled out, what has not been ruled out, and what the next safe step should be.
Here are the questions I would want my wife to have in her hand if she was still in pain after a normal ultrasound:
- “What exactly did my ultrasound look for?”
- “Does this scan rule out endometriosis, or only certain types of endometriosis?”
- “Could superficial peritoneal endometriosis still be present even if my scan is normal?”
- “Was my scan performed or reviewed by someone with specialist experience in endometriosis imaging?”
- “Do my symptoms suggest deep endometriosis, bowel involvement, bladder involvement, adenomyosis, pelvic floor dysfunction, or another cause of chronic pelvic pain?”
- “Would a specialist transvaginal ultrasound or MRI be appropriate in my case?”
- “Should I be referred to a gynaecologist or an endometriosis specialist centre?”
- “What should we do if treatment does not improve my symptoms?”
- “Could hormonal treatment help my symptoms, and what are the benefits, risks, and side effects for me personally?”
- “What are my options if I am trying to conceive or worried about fertility?”
- “Would pelvic floor physiotherapy, pain management, or a chronic pelvic pain clinic be worth considering?”
- “At what point would laparoscopy be considered if imaging stays normal but symptoms continue?”
These questions matter because they move the appointment away from one sentence, “your scan is normal,” and towards a fuller conversation. NICE recommends specialist ultrasound or MRI for suspected deep endometriosis when appropriate, and also says laparoscopy can be considered to diagnose suspected endometriosis even when ultrasound or MRI is normal.
Please also ask your doctor to explain things in plain English. You are allowed to say, “Can you tell me what that means for my daily life?” or “Can you write down the plan, because I am overwhelmed and I do not want to forget?”
If you feel dismissed, try to stay calm but firm. You can say, “I understand the scan is normal, but my symptoms are still affecting my life. What is the next step if endometriosis is still possible?”
That one sentence can help protect you. It does not attack the doctor, but it makes it clear that your pain has not disappeared just because the scan report looks tidy.
I wish every woman had a partner beside her who remembered the details when she was too tired to speak. I wish every man understood that support is not taking over the appointment, but sitting there as quiet proof that she is not exaggerating, not alone, and not going to be left to carry the whole weight of being believed by herself.
Final Word on Normal Ultrasound But Still Endometriosis Pain
If you take one thing from this article, let it be this: a normal scan can be useful information, but it is not the same as a complete explanation for your pain. It may reduce concern about some visible problems, but it does not automatically rule out endometriosis, especially superficial disease or symptoms that need specialist assessment.
NICE guidance is clear that endometriosis should not be excluded simply because the examination and ultrasound are normal, and ESHRE also warns that negative imaging does not exclude the disease, particularly superficial peritoneal endometriosis.
That matters because your body is not asking for attention without reason. When pain keeps returning, when your period controls your calendar, when bowel movements become frightening, when sex becomes painful, when fatigue flattens you, or when you start shrinking your life around symptoms, something deserves to be explored properly. Not because you are anxious. Not because you are dramatic. Because pain that changes your life is information.
I have learned this through loving my wife. I have seen how easily a woman can begin to question herself when results come back “normal” but her body still feels unsafe, unpredictable, and exhausting. I have seen the way one short appointment can either give a little hope or leave her feeling like she has to prove her suffering all over again.
And that is why I want you to hear this in a human voice, not a cold clinical sentence. You are allowed to ask what the ultrasound could see. You are allowed to ask what it could not see. You are allowed to ask whether you need specialist imaging, a gynaecology referral, pain support, pelvic floor assessment, or further investigation.
NICE says referral may still be necessary even with a normal scan, especially when symptoms continue, or initial treatment is not effective, tolerated, or suitable.
You are also allowed to bring someone with you. A partner, friend, sister, mother, or anyone who can help you remember the details when pain and nerves make your mind go blank. If you are the partner reading this, please understand that belief is not a small thing. Sometimes your steady, quiet “I believe you” becomes the safest place she has while the medical system is still trying to catch up.
Endometriosis is not only about what shows up on a screen. WHO describes it as a chronic disease that can cause severe period pain, chronic pelvic pain, heavy bleeding, bloating, nausea, infertility, and symptoms beyond the pelvis in some cases. It can touch confidence, intimacy, work, fertility, mental health, and the way a woman feels inside her own body.
So please do not let one normal report become the end of your story if your symptoms are still taking pieces of your life. Let it become the beginning of better questions, better documentation, better support, and better care. You deserve answers that match the reality you are living, not reassurance that only looks good on paper.
You are not difficult for wanting clarity. You are not weak for being tired. You are not wrong for knowing your body is still asking for help.
A normal scan can miss parts of the story, but your lived experience still counts. Keep tracking your symptoms, keep asking careful questions, and keep looking for care that treats your pain as real. You deserve to be believed, supported, and guided with compassion, not left alone with confusion.
Please leave a comment below if this spoke to you, and check out the FREE chapter of my eBook at the bottom of this post if you need more validation, support, and gentle guidance for life with endometriosis.


About Me
Hi, I’m Lucjan! The reason why I decided to create this blog was my beautiful wife, who experienced a lot of pain in life, but also the lack of information about endometriosis and fibromyalgia for men…
READ MORE
Grab a FREE eBook!
“You Did NOTHING To Deserve This!”
Finally hear the words nobody ever said to you, that your pain is real, your tears make sense, and you did nothing to deserve endometriosis, the dismissal, or the way it has rewritten your life.
Related Questions You May Be Asking About Normal Ultrasound But Still Endometriosis Pain
1. Can endometriosis be missed on ultrasound?
Yes, endometriosis can be missed on ultrasound, especially if the disease is superficial, small, hidden behind organs, or not looked for by someone trained in specialist pelvic imaging. Ultrasound can be helpful, but it does not see everything. If your symptoms still fit endometriosis, a normal scan should not automatically end the conversation.
2. Does a normal pelvic scan mean my pain is not serious?
No, a normal pelvic scan does not mean your pain is not serious. It may mean nothing obvious was seen on that test, on that day, with that method. Pain that affects your periods, bowel, bladder, sex life, sleep, work, or emotional wellbeing still deserves proper review, because your daily life matters as much as the report.
3. What type of endometriosis is hardest to see?
Superficial peritoneal endometriosis is often harder to see on standard imaging because it can appear as small, flat, scattered lesions on the pelvic lining. Deep endometriosis and ovarian endometriomas may be easier to detect in skilled hands, but even then, imaging depends on training, technique, and what areas are assessed.
4. Should I ask for an MRI after a normal ultrasound?
An MRI may be useful if your symptoms suggest deep endometriosis, bowel involvement, bladder involvement, adenomyosis, or complex pelvic disease. It is not always the next step for everyone, but it can help in the right situation. I would ask your doctor what your ultrasound could not rule out and whether specialist imaging makes sense for you.
5. When is laparoscopy considered if scans are normal?
Laparoscopy may be considered when symptoms strongly suggest endometriosis, imaging is normal, and pain continues despite treatment or reassurance. It is a surgical procedure, so it should be discussed carefully, including benefits, risks, recovery, and alternatives. But for some people, it becomes the step that finally gives answers after years of confusing symptoms.
6. How can I explain this to my partner?
Tell your partner that a normal scan does not always mean there is no disease, and that you need belief, patience, and practical support while answers are still being explored. Share your symptoms clearly: what happens, when it happens, and how it changes your life. The right partner should not wait for perfect proof before offering compassion.
Normal Ultrasound But Still Endometriosis Pain References
- https://www.nice.org.uk/guidance/ng73
- https://www.nice.org.uk/guidance/ng73/chapter/recommendations
- https://www.nice.org.uk/guidance/ng73/resources/visual-summary-on-first-presentation-initial-management-diagnosis-referral-and-ongoing-care-of-pdf-13559822461
- https://www.eshre.eu/Guidelines-and-Legal/Guidelines/Endometriosis-guideline
- https://www.who.int/news-room/fact-sheets/detail/endometriosis
- https://www.nhs.uk/conditions/endometriosis/
- https://www.nhs.uk/symptoms/pelvic-pain/
- https://www.rcog.org.uk/for-the-public/browse-our-patient-information/bleeding-andor-pain-in-early-pregnancy/
- https://www.mayoclinic.org/diseases-conditions/endometriosis/symptoms-causes/syc-20354656
- https://en.wikipedia.org/wiki/Endometriosis