Are You Told Endo Bladder Pain Is Just a UTI?
Have you been told endo bladder pain is just a UTI, even though the burning, pressure, or urgency keeps returning around your period? If so, there’s a chance you experienced endometriosis medical gaslighting.
You may be exhausted from repeating the same symptoms, while each appointment begins as if the last one never happened. If treatment has not settled the pattern, you are not being difficult for asking what else needs to be considered.
Bladder pain can come from a UTI, but repeated or cyclical urinary pain may also be linked to endometriosis affecting the bladder. Infection should be checked with appropriate urine testing, while persistent symptoms deserve a full endometriosis-aware assessment rather than automatic antibiotics.
I am not a clinician, but I write as a medically trained husband, blogger and researcher, and I have placed the NHS, NICE, ESHRE and study sources used for the medical context at the bottom.
Urinary tract endometriosis is uncommon overall, yet estimates vary widely because some cases cause no obvious urinary symptoms. In a major clinical review, the bladder was the most frequently affected urinary site, while roughly half of those with urinary tract involvement may have no symptoms.
That matters because pain when you pee, urgency, frequency, and even blood in the urine can overlap with infection. A menstrual pattern can be a valuable clue, but symptoms do not have to follow a perfect calendar, and a real UTI can still occur alongside endometriosis.
Watching my wife explain changing symptoms taught me that a familiar label can feel comforting to a rushed room while leaving the person in pain completely unheard. I learned to listen for the pattern, not merely the name attached to one appointment.
Let us look at what can separate infection from an endometriosis-related bladder problem, what deserves further investigation, and how you can ask for that help without apologising for needing it.
- Why Being Told Endo Bladder Pain Is Just a UTI Can Delay Answers?
- How to Investigate Being Told Endo Bladder Pain Is Just a UTI?
- How Being Told Endo Bladder Pain Is Just a UTI Affects Both of You?
- When to Seek Medical Help?
- Questions to Ask Your Doctor
- Final Word on Being Told Endo Bladder Pain Is Just a UTI
- FREE eBook
Why Being Told Endo Bladder Pain Is Just a UTI Can Delay Answers?
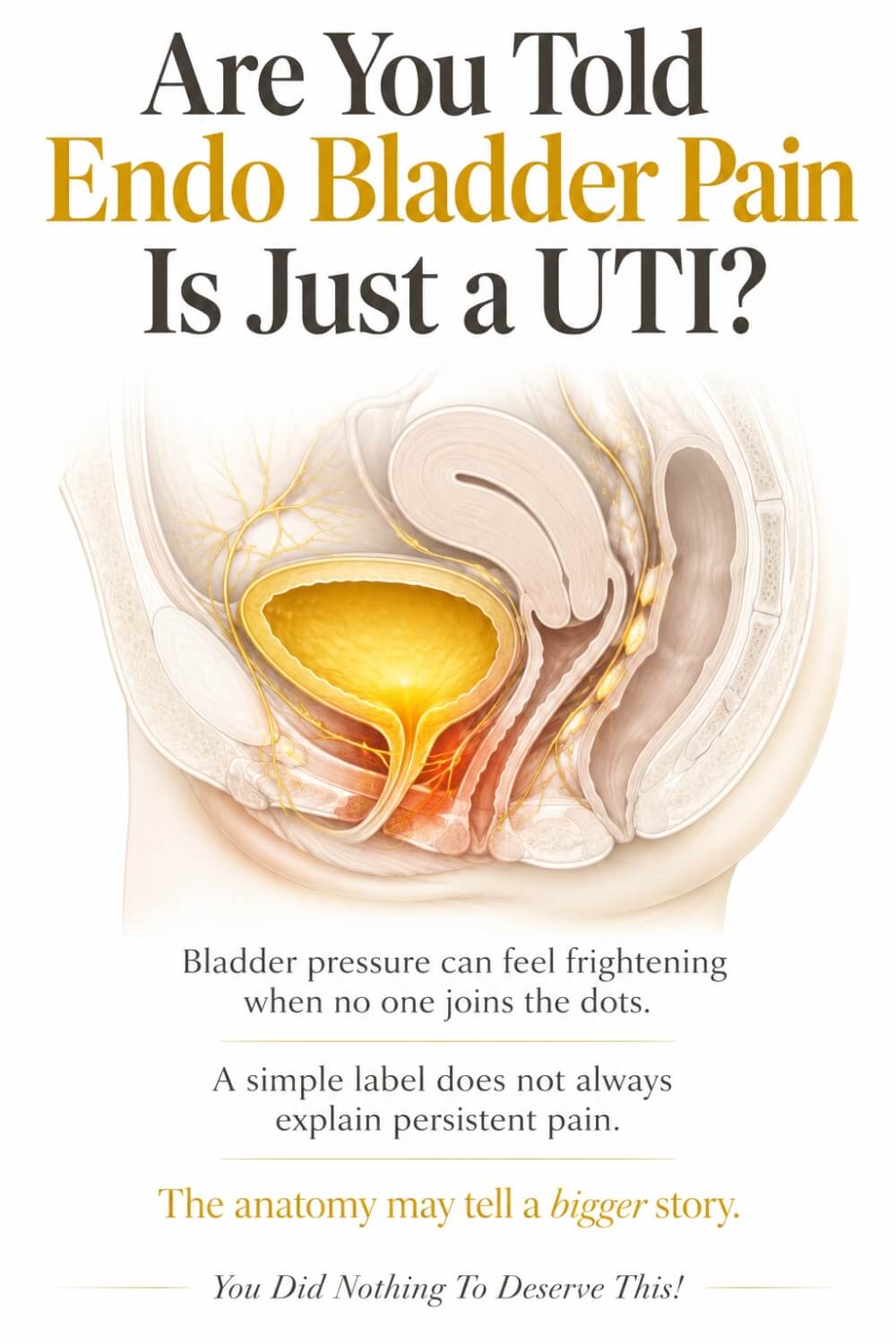
When you are told endo bladder pain is just a UTI, the conclusion may sound plausible because both problems can cause burning, urgency, frequency, and lower abdominal discomfort. A UTI is usually an infection somewhere in the urinary tract, whereas bladder endometriosis involves endometriosis affecting or growing into tissue around the bladder, often its muscular wall.
The overlap means symptoms alone cannot safely prove either explanation. It also means one negative urine result does not automatically diagnose endometriosis, just as one past infection does not explain every future flare.
Timing can add valuable context. Pain, painful urination or blood in the urine that repeatedly worsens around menstruation is specifically recognised in UK guidance as a reason to suspect endometriosis.
Still, bladder symptoms can occur outside a neat monthly window. Long-standing inflammation, pelvic floor guarding, nerve sensitisation and disease at neighbouring pelvic sites may blur the pattern.
A useful assessment therefore looks at the whole history, not one dipstick or one day of symptoms. Culture results, response to antibiotics, cycle timing, bladder filling, sex, pelvic pain and previous endometriosis findings all help build a clearer picture.
NICE recommends transvaginal ultrasound for suspected endometriosis, including a search for deep disease involving the bladder or ureter. That scan is most helpful when the person performing and interpreting it has specialist endometriosis imaging expertise.
A normal examination or ultrasound does not close the case. NICE is clear that endometriosis should not be excluded solely because those results are normal, and specialist ultrasound or pelvic MRI may be considered when deep disease is suspected.
The ureters matter too because they carry urine from the kidneys to the bladder. Ureteral endometriosis can sometimes obstruct urine flow quietly, which is why suspected deep urinary disease belongs in a specialist service with gynaecology, imaging and urology expertise.
The hardest part for me has never been accepting that clinicians must rule out common causes first. It is seeing what happens inside the woman I love when “common” becomes “case closed” and her unfinished pain is handed back to her.
If that has happened to you, the next steps are not about proving anyone wrong; they are about helping your clinical team see the pattern clearly:
- Record symptoms beside your cycle
- Ask what urine testing showed
- Note treatment and symptom response
- Describe bladder pain precisely
- Bring your endometriosis history
- Request endometriosis-aware imaging
- Ask about other possible causes
- Know when referral is appropriate
Record Symptoms Beside Your Cycle
A symptom diary is not proof of a diagnosis, but it can turn a fog of painful days into a pattern your clinician can examine. Record the date, where you are in your menstrual cycle, pain intensity, burning, urgency, frequency, night-time trips, visible blood and whether a full bladder or passing urine changes the pain. Add pelvic pain, painful sex, bowel symptoms and bleeding only when they occur, rather than trying to make every symptom fit.
Also record fever, chills, cloudy urine and pain beneath the ribs because these may point towards infection or kidney involvement and should not be folded into an endometriosis theory.
NICE says a pain and symptom diary can aid discussions, and ESHRE notes that it may help make symptoms more visible during history-taking. You are not building a legal case against your doctor. You are giving both of you a clearer map than memory can provide during a short, stressful appointment.
Ask What Urine Testing Showed
It is reasonable to ask whether your urine was assessed, what type of test was used, and whether a laboratory culture was needed. A dipstick may support an initial decision, while a culture looks for bacterial growth and can help guide antibiotics, but the right testing depends on your circumstances and clinical judgement.
Do not treat a negative result as automatic proof of bladder endometriosis, because chronic UTI and several non-infectious conditions can also produce persistent urinary symptoms.
Equally, repeated treatment without a clear review deserves a calm question: “What evidence suggests infection this time, and what will we consider if the test is negative or treatment does not help?”
Blood in the urine needs proper assessment rather than being assigned to either endometriosis or infection without thought. Asking for the result is not challenging the clinician’s authority. It is shared decision-making about your own body.
Note Treatment and Symptom Response
Write down the name and dates of any antibiotic, pain medicine, or hormonal treatment, plus what changed and what did not. If burning eased within treatment but the same pressure returned with the next period, that detail matters. If nothing improved, that matters too, although lack of response alone cannot identify the cause because the antibiotic, organism, dose, adherence, or original diagnosis may all need review.
Include side effects and whether symptoms returned immediately or after a symptom-free gap. Never stop prescribed antibiotics early or reuse leftovers without professional advice, and do not assume every flare needs another course.
A careful treatment history can prevent the next appointment becoming another blank beginning. It gives your clinician a chance to separate a documented infection, an uncertain episode, and a repeating pelvic pattern instead of treating them as the same event.
Describe Bladder Pain Precisely
“Bladder pain” can mean burning at the urethra, pressure behind the pubic bone, cramping as the bladder fills, pain while urine passes, or an ache that remains afterwards.
Tell the clinician which description fits, when it begins, how long it lasts, and whether emptying your bladder relieves or worsens it. Mention urgency, frequency, leakage, difficulty starting, incomplete emptying, and waking at night, but only if you actually experience them.
Use ordinary words before medical terms because clarity matters more than sounding clinical. You might say, “As my bladder fills, the pressure behind my pubic bone rises, and it becomes sharp when I pee during the first two days of my period.” That is more useful than saying only that your UTI is back.
Precise language keeps the investigation open to infection, bladder or ureter endometriosis, bladder pain syndrome, stones, pelvic floor problems, and other causes that require a clinician to distinguish.
Bring Your Endometriosis History
Bring a short timeline of when pelvic and urinary symptoms began, any diagnosis already made, previous scans, operations, pathology reports, and treatments. If surgery found deep disease near the front of the pelvis, bladder, ureters or uterovesical space, include the exact wording rather than relying on memory.
Previous endometriosis does not prove that every urinary symptom comes from it, but it changes the context in which recurring symptoms should be assessed.
If you can access NHS records or clinic letters, place the most relevant pages at the front. Add a one-page summary so the clinician is not expected to search through a thick folder during a brief appointment.
I learned this while helping my wife: preparation should reduce her burden, not become another job that consumes the little energy she has. A partner can organise dates or take notes, but your voice, consent and priorities must remain at the centre.
Request Endometriosis-Aware Imaging
NICE recommends a transvaginal ultrasound for suspected endometriosis even when the pelvic examination is normal, with attention to deep disease involving the bladder or ureter. A standard pelvic scan and a specialist endometriosis scan are not always equivalent.
The referral should make the clinical question visible, because the examiner may need to assess the bladder wall, pelvic ureters, organ mobility and other deep-disease sites deliberately.
You can ask, “Will this scan be performed and interpreted by someone experienced in deep endometriosis, and will the bladder and ureters be assessed?” Specialist ultrasound or pelvic MRI may be used to map suspected deep disease and plan care. A normal result can be reassuring about what was seen, but it does not automatically exclude endometriosis. If symptoms remain significant, ask what the normal scan rules out, what it cannot rule out, and what the next step will be.
Ask About Other Possible Causes
Good care does not replace the label “UTI” with “endometriosis” before evidence is gathered. Ask what else could explain your symptoms, including recurrent or chronic UTI, bladder pain syndrome, urinary stones, pelvic floor dysfunction, urethral conditions and, when blood is present, other urinary tract disease.
The purpose is not to collect frightening possibilities. It is to stop one familiar explanation from becoming the only explanation.
Some conditions can coexist, and pain may have more than one contributor. A clinician may need urine testing, examination, imaging, or referral to narrow the list safely. If you hear “your urine is clear”, a useful response is, “Thank you. Since the pain continues, what non-infectious causes are we considering?” That keeps the conversation calm and forward-looking.
You deserve a differential diagnosis, which simply means a reasoned list of possibilities, not a dismissal because the easiest one was not confirmed.
Know When Referral Is Appropriate
NICE advises gynaecology referral when symptoms persist, recur, affect daily life or do not respond to initial treatment. Suspected or confirmed deep endometriosis involving the bladder or ureter should be referred to a specialist endometriosis service.
Such a service should have access to advanced gynaecological imaging and a urologist with an interest in endometriosis, because urinary tract disease can require coordinated decisions.
You can ask directly, “Do my cyclical urinary symptoms and endometriosis history meet the criteria for specialist referral?” If the answer is no, ask what criteria are missing, what will be tried next, and when the decision will be reviewed. Referral is not a promise that bladder endometriosis will be found, and it is not always the first step.
It is a route to the right expertise when the pattern, severity, or suspected disease depth is beyond routine management.
How to Investigate Being Told Endo Bladder Pain Is Just a UTI?
Once you have been told endo bladder pain is just a UTI, the safest next step is not to choose your preferred diagnosis but to test the reasonable possibilities in a structured way. The first question is whether infection is likely now and whether your circumstances call for urine testing or culture.
A sample collected while you have symptoms may provide more useful evidence than a vague recollection from months earlier. If bacteria are identified, the result may guide treatment, while persistent symptoms after treatment still deserve review.
Visible or confirmed blood in urine should be investigated rather than assumed to come from menstruation or endometriosis. Your clinician also needs to know about fever, chills, flank pain, pregnancy, kidney problems and difficulty passing urine because these details can change urgency.
For suspected endometriosis, NICE now recommends transvaginal ultrasound even when an examination is normal. The request should state the concern about deep disease so the bladder and ureters are assessed deliberately.
Routine imaging can miss small lesions or disease outside the area examined. A normal ultrasound therefore cannot, by itself, erase a consistent clinical history.
Specialist ultrasound or pelvic MRI may help assess the location and extent of deep disease before treatment or surgery. Cystoscopy can sometimes help when blood has been confirmed, or imaging shows a bladder nodule, although bladder-wall disease may sit beneath apparently normal inner lining.
Suspected deep bladder or ureter disease belongs in a specialist endometriosis service with access to a urologist and expert imaging, which is the pathway described in UK guidance rather than an excessive request.
When my wife entered appointments already braced to defend what she felt, I saw how quickly healthcare could become something she had to survive rather than use. The most loving thing I could do was help carry the records, remember the questions, and make sure a disappointing test result did not turn into the false message that her pain was imaginary.
How Being Told Endo Bladder Pain Is Just a UTI Affects Both of You?
Repeatedly being told endo bladder pain is just a UTI can make you doubt your memory, especially when every short appointment captures only one day of a repeating cycle. You may begin rationing drinks, planning every journey around toilets or fearing that intimacy will trigger another flare.
Your partner may see the practical damage without understanding the sensation inside your body. His job is not to diagnose the cause or promise that it must be endometriosis.
He can believe the pain, help record patterns, attend appointments with consent, and ask what the next step is if infection is not confirmed. He should also avoid turning support into interrogation by asking you to prove every symptom at home.
For me, support means noticing when my wife has spent all her energy explaining and taking over the tasks that do not require her voice. It means remembering that a cancelled plan is not rejection and that pain does not need a laboratory result before compassion is allowed.
Treatment depends on what clinicians find, your priorities and whether fertility matters to you. Confirmed infection may require antibiotic care, while suspected or confirmed endometriosis may be managed with pain relief, hormonal options, monitoring or specialist surgery, particularly if deep disease threatens urinary flow.
No partner can remove that uncertainty, but he can stop you carrying it alone. When the two of you treat the problem as something to face together, the relationship becomes a place where your reality is protected rather than questioned again.
When to Seek Medical Help?
Arrange a routine GP appointment if urinary burning, urgency, frequency, or bladder pressure keeps returning, follows your menstrual cycle, affects sleep or daily life, or continues despite treatment. Take your symptom diary and ask for both infection and non-infectious causes to be considered.
Seek prompt advice from a GP, urgent service or NHS 111 if symptoms worsen quickly, do not improve within 48 hours of starting UTI treatment, or keep returning. NHS guidance defines recurrent UTI as two episodes within six months or three within twelve months, which also warrants medical review.
Get urgent advice if you have blood in your urine, pain in your lower tummy or back beneath the ribs, a very high or low temperature, shivering, pregnancy, diabetes, a weakened immune system or a catheter. These features can occur for several reasons and should not be assumed to be endometriosis.
Seek urgent assessment if you cannot pass urine, develop severe flank pain, are vomiting or feel seriously unwell. Call 999 or go to A&E if you become confused, very drowsy or have difficulty speaking, as these can be signs of a serious systemic illness.
Even when your symptoms have a strong cycle pattern, a new UTI or kidney infection is still possible. You deserve care that can hold both truths: endometriosis should not be dismissed, and potentially urgent urinary illness should not be missed.

Questions to Ask Your Doctor
You do not need to ask every question below. Choose the ones that match your symptoms and place the most important three at the top.
- “What makes infection the leading explanation this time, and was a urine culture needed?”
- “Could I see or receive the urine test and culture results?”
- “If this is a UTI, when should I expect improvement and what happens if I do not improve?”
- “Because this pain repeats around my period, could endometriosis involving or irritating the bladder be considered?”
- “What other causes of persistent urinary pain are on your differential diagnosis?”
- “Would a transvaginal ultrasound be appropriate, and will it assess the bladder and ureters for deep endometriosis?”
- “Will the scan be performed or reviewed by someone experienced in specialist endometriosis imaging?”
- “If the scan is normal but symptoms continue, what would the next step be?”
- “Do the urinary symptoms or my history justify pelvic MRI, urology input or referral to a specialist endometriosis service?”
- “Do I need kidney imaging or renal function tests if ureter involvement is a concern?”
- “What should make me seek urgent help rather than wait for the next appointment?”
Bring a short description of your pattern and let the clinician read it before the discussion moves on. If you feel rushed, ask for the plan to be written down, including what is being ruled out, what treatment is being tried and when it will be reviewed.
Final Word on Being Told Endo Bladder Pain Is Just a UTI
If urinary pain has repeatedly been called an infection, you may have learned to enter every appointment already defending yourself. That reaction does not mean you are hostile, dramatic or obsessed with endometriosis. It may mean you have spent too long receiving a familiar answer without a plan for what happens when that answer does not fit.
A UTI remains a real possibility whenever burning, urgency, frequency or lower abdominal pain appears. It deserves appropriate assessment because infection can worsen and, in some circumstances, reach the kidneys. Endometriosis does not protect you from infection, and a cycle pattern should never be used to ignore fever, flank pain, blood in your urine or feeling seriously unwell.
The reverse matters just as much. A previous UTI does not prove that each returning bladder flare has the same cause. UK guidance recognises cyclical pain passing urine and blood in urine as symptoms that should raise suspicion of endometriosis. It also recommends ultrasound for suspected disease, specialist imaging when deep involvement is possible and referral to an endometriosis service when the bladder or ureter may be affected.
That pathway is not about demanding a particular diagnosis. It is about asking for infection, endometriosis and other urinary or pelvic causes to be considered with equal care. Good medicine can hold uncertainty without handing the uncertainty back to you as blame.
The answer may come from a culture, a scan, an MRI, a specialist review or several steps considered together. Sometimes the conclusion will not be bladder endometriosis, and that does not make the investigation wasted. Ruling out one cause can guide care towards another. What matters is that each result changes the plan, rather than becoming another reason to leave you alone with pain that still needs explaining.
Keep a clear diary, obtain your test results, and record what treatment changed. Explain where the pain sits, whether bladder filling affects it and how it relates to bleeding or your menstrual cycle. Ask what a normal result rules out, what it cannot rule out, and when the next review will happen.
If you are told endo bladder pain is just a UTI, you can respond calmly: “I understand why infection is being considered. Because this keeps returning and follows this pattern, what is our plan if testing is negative or treatment does not resolve it?” That sentence respects clinical judgement without surrendering your own experience.
I have watched my wife spend strength she did not have trying to make invisible pain understandable. My role was never to speak over her or decide what her body meant. It was to believe her, help preserve the details and stand beside her while the right questions were asked.
You deserve that steadiness too. Your pain needs careful investigation, not automatic certainty. Your records, patterns and questions are useful clinical information. Most importantly, a test that does not reveal the answer is not evidence that you invented the problem. It only means the search must remain thoughtful, proportionate and human.
Your recurring bladder pain deserves more than a repeated label. Infection should be checked safely, endometriosis should be considered when the pattern fits, and persistent symptoms need a clear next step. You are not overreacting by asking what the evidence shows and what happens if the first explanation is wrong.
If this reflects something you have lived through, leave a comment, and please see my free 130+ page eBook at the bottom of this post for more validation and support.


About Me
Hi, I’m Lucjan! The reason why I decided to create this blog was my beautiful wife, who experienced a lot of pain in life, but also the lack of information about endometriosis and fibromyalgia for men…
READ MORE
Grab a FREE eBook!
“You Did NOTHING To Deserve This!”
Finally hear the words nobody ever said to you, that your pain is real, your tears make sense, and you did nothing to deserve endometriosis, the dismissal, or the way it has rewritten your life.
Related Questions You May Be Asking About Being Told Endo Bladder Pain Is Just a UTI
Can bladder endometriosis cause symptoms that feel like a UTI?
Yes. Bladder endometriosis can be associated with painful urination, urinary frequency, urgency, pelvic or bladder pain and sometimes blood in the urine. Those symptoms overlap with infection, so the feeling alone cannot identify the cause. A clinician may use your history, urine testing and specialist imaging to investigate safely.
Can a negative urine test confirm bladder endometriosis?
No. A negative dipstick or culture may make some infections less likely, but it does not diagnose endometriosis. Persistent urinary symptoms can have several causes, including chronic UTI, bladder pain syndrome, stones, pelvic floor dysfunction or deep endometriosis. The result should guide the next clinical question rather than end the investigation.
Must bladder endometriosis symptoms happen only during periods?
No. A cyclical pattern is an important clue and is recognised in endometriosis guidance, but symptoms may also occur between periods or become more constant. Pain patterns can be influenced by disease location, inflammation, pelvic floor tension and pain sensitisation. Record timing honestly instead of forcing symptoms into a perfect monthly pattern.
What imaging may detect endometriosis involving the bladder?
NICE recommends transvaginal ultrasound for suspected endometriosis and says it should look for deep disease involving the bladder or ureter. Specialist ultrasound or pelvic MRI may help map suspected deep disease. A normal scan does not automatically exclude endometriosis, so ongoing significant symptoms may still justify referral or further assessment.
Can a UTI and endometriosis occur at the same time?
Yes. Having endometriosis does not prevent a bacterial urinary infection, and having a confirmed UTI does not explain every later episode. New fever, shivering, flank pain, worsening illness or blood in the urine requires medical attention. Clinicians may need to treat infection while separately reviewing a recurring or cycle-linked pelvic pattern.
Being Told Endo Bladder Pain Is Just a UTI References
- https://www.nice.org.uk/guidance/ng73/chapter/Recommendations
- https://www.nhs.uk/conditions/endometriosis/
- https://www.nhs.uk/conditions/urinary-tract-infections-utis/
- https://www.eshre.eu/-/media/sitecore-files/Guidelines/Endometriosis/ESHRE-GUIDELINE-ENDOMETRIOSIS-2022_1.pdf
- https://www.rcog.org.uk/for-the-public/browse-our-patient-information/endometriosis/
- https://www.mdpi.com/2075-4418/10/10/771
- https://www.endometriosis-uk.org/getting-diagnosed-0